
From the 1Service de Médecine Physique et de Réadaptation, AP-HP, Hôpital Fernand Widal, Université Paris Diderot, 2Cognition and Action Group, Cognac-G, CNRS UMR 8257, Université Paris Descartes, 3Service de Physiologie Clinique-Explorations Fonctionnelles, AP-HP, Hôpital Lariboisière, INSERM UMR965, Université Paris Diderot, Sorbonne Paris Cité, and 4Service d’Immuno-Hématologie, AP-HP, Hôpital Saint-Louis, Paris, France
Objective: To investigate the weight of visual and proprioceptive inputs, measured indirectly in standing position control, in patients with chronic acquired demyelinating polyneuropathy (CADP).
Design: Prospective case study.
Subjects: Twenty-five patients with CADP and 25 healthy controls.
Methods: Posture was recorded on a double force platform. Stimulations were optokinetic (60°/s) for visual input and vibration (50 Hz) for proprioceptive input. Visual stimulation involved 4 tests (upward, downward, rightward and leftward) and proprioceptive stimulation 2 tests (triceps surae and tibialis anterior). A composite score, previously published and slightly modified, was used for the recorded postural signals from the different stimulations.
Results: Despite their sensitivity deficits, patients with CADP were more sensitive to proprioceptive stimuli than were healthy controls (mean composite score 13.9 ((standard deviation; SD) 4.8) vs 18.4 (SD 4.8), p = 0.002). As expected, they were also more sensitive to visual stimuli (mean composite score 10.5 (SD 8.7) vs 22.9 (SD 7.5), p < 0.0001).
Conclusion: These results encourage balance rehabilitation of patients with CADP, aimed at promoting the use of proprioceptive information, thereby reducing too-early development of visual compensation while proprioception is still available.
Key words: balance; polyneuropathy; visual stimulation; proprioceptive stimulation.
Accepted Nov 24, 2017; Epub ahead of print Jan 9, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Clément Provost, Hôpital Fernand Widal, service MPR, 200, rue du Faubourg Saint-Denis, FR-75010, Paris, France. E-mail: clementprovost@yahoo.fr
Proprioception can be defined as the sense of self-perception of body and limb orientation, position and motion (1). Disorders affecting proprioception, such as peripheral polyneuropathies, are frequent and could benefit from rehabilitation. Patients with chronic acquired demyelinating polyneuropathy (CADP) (2) usually present proprioceptive impairment, which leads to difficult postural reweighting with increased risk of falls (3). This deficit in proprioception induces adapted or misfit compensation, commonly defined as reliance on visual information during balance (4).
CADP represents a heterogeneous group of immune-mediated polyneuropathies with an incidence of approximately 6/100,000 people. The conditions include chronic inflammatory demyelinating polyneuropathy (CIDP), anti-myelin-associated glycoprotein neuropathy (anti-MAG neuropathy), multifocal motor neuropathy, and neuropathy associated with polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes (POEMS) syndrome. Different characteristic phenotypes for these 4 types of neuropathy have been identified.
Because of a particular interest of our hospital, this study focused on patients with CIDP and anti-MAG neuropathy presenting ataxia (5). CIDP is both a proximal and distal sensory-motor, often symmetrical, neuropathy. Ataxia is present in 10–15% of patients with CIDP (6). Anti-MAG neuropathy is usually characterized by symmetrical limb weakness and sensory deficit, mostly distal. Anti-MAG neuropathy is a slowly progressive, predominantly sensory neuropathy with ataxia and distal paraesthesia. In nerve conduction studies, patients with these 2 diseases show signs of demyelination (7).
To maintain balance, the central nervous system (CNS) continuously integrates sensory information and has to make choices in case of sensory conflict. Visual, vestibular and proprioceptive afferents are involved in providing the CNS with feedback about the body segment positions and their correlation with each other and the surroundings (8). When vision, vestibule or proprioception is altered, a possible compensation strategy to help maintain balance during standing is sensory reweighting of the information from these systems (9). According to this strategy, the CNS identifies the less reliable information from one sensory system, thereby reducing its weight and relying on the others. However, failure of the compensation strategies may result in impaired standing balance with consequent increased risk of falls (10).
A previous study observed that diminished proprioception of patients with polyneuropathy could be well compensated by vision (11). Nevertheless, other authors observed that postural stability in diabetic patients with polyneuropathy could be altered even with compensated vision (12). The compensation of proprioceptive impairments by vision can be excessive or inappropriate (13), leading to visual dependence. Visual dependence is defined as the preponderance of the use of visual cues, even with impaired vision, despite normal vestibular and proprioceptive cues. This comportment can be observed among healthy people (14) and has been described in different pathological conditions, such as stroke (13).
Postural strategies occurring after stroke have been studied on a force platform with centre of pressure (CoP) displacement during proprioceptive, visual and vestibular perturbations (15). We aimed to investigate the weight of visual and proprioceptive inputs (measured indirectly in standing position control) in CADP and healthy participants, and study the relation of the inputs to clinical motor and sensory scores. We used the same method previously published for stroke patients. The hypothesis was that patients with CADP with ataxia, with their sensitivity deficit, may be less sensitive to proprioceptive information and more sensitive to visual information than healthy people.
Patients with CADP were recruited in our Department of Clinical Physiology. Inclusion criteria were age > 18 years, CIDP or anti-MAG neuropathy, and ataxia evaluated by Mariette score (16). Exclusion criteria were: patients with other neurological histories, who were unable to remain standing on a stabilometric platform or had a Medical Research Council (MRC) score <40 (see the paragraph, below, on clinical assessment). Healthy controls were recruited from the staff of our Department of Physical and Rehabilitation Medicine.
Right and left inferior limb muscle strength was assessed by the MRC score on 5 muscles (tibialis anterior, triceps surae, extensor hallucis longus, peroneus longus, quadriceps). Scores ranged from 0 for no detectable contraction to 5 for normal strength for each muscle, for a maximum strength score of 50. Sensitivity impairment was assessed on left and right feet for pain, pallesthesia sensitivity (diapason) and joint position sense of the hallux. Scores were 0 for anaesthesia, 1 for hypoaesthesia, and 2 for normal sensitivity for each test, for a maximum sensitivity score of 12.
Posture was examined by use of a double force platform (FeeTest 2, TechnoConcept®, Mane, France) consisting of 2 force platforms, each with 4 force transducers that recorded the vertical ground reaction forces. Participants were asked to stand at ease, with their feet parallel and 15 cm apart, looking straight ahead with their head erect and their arms hanging by their sides. The variation in position of the CoP was calculated in millimetres by using the software Posturewin (TechnoConcept®, Mane, France) and separated into 2 signals, the anteroposterior signal and mediolateral signal. Data were collected at a sampling frequency of 40 Hz.
Before stimulations, a Romberg score (17) was calculated from the first 2 tests of 35 s each. The Romberg score was the quotient between the recorded statokinesigram area for the CoP displacement with eyes closed and the area with eyes open multiplied by 100.
The experiment lasted approximately 30 min (15). Six different tests were successively performed in the same order for all participants. Each test began with a 15-s baseline pre-period, with no stimulation, followed by a 35-s per-period stimulation, for a total duration of 50 s for each test.
Proprioceptive input stimulation involved the use of electromechanical vibrators (VB115, TechnoConcept®, Mane, France) that were adjusted manually and were perpendicular to the tendon of the muscles to be stimulated. Each cylindrical vibrator was 7 cm long and 3 cm in diameter. Mechanical vibrations (pulse duration: 5 ms, amplitude: 1 mm peak to peak) were delivered at 50 Hz. Two tests were performed: the first with vibrators placed on triceps-surae distal tendons on each side, the second with vibrators placed on tibialis-anterior distal tendons on each side. The duration and frequency of the stimulation were controlled by the software Multivibra (TechnoConcept®, Mane, France). Vibratory stimulation was applied in a lighted room, with the participant’s eyes open.
Visual input stimulation involved the use of an optokinetic device in a dark room without any visual reference cues. Optokinetic stimulation was induced by numerous luminous spots produced by a rotating sphere (Optotest, TechnoConcept®, Mane, France; speed of rotation 60°/s) that was placed just above the participant’s head, with the spots moving along a smooth wall in front of the participant. Participants were instructed to stare straight ahead without any fixed-in-space visual target and without attempting to follow the moving dots with the eyes. Four visual stimulations were tested, once each: upward, downward, leftward and rightward.
Displacement of the CoP (mm) during the proprioceptive and visual stimulation tests were separated into anteroposterior and mediolateral signals and analysed by the following equations. Relative displacement of the CoP during stimulation (from seconds 15 to 50) was first calculated as displacement of the CoP during stimulation minus the mean position of the CoP in the initial resting period (from seconds 2 to 13) (a). Then, the score was obtained by computing the mean relative displacement of the CoP during stimulation (b). This score was computed for each direction (anterior, posterior, right and left) for each test in each type of sensorial stimulation (proprioceptive and visual) and expressed in absolute value.
where Y is the signal in the anteroposterior axis. A positive Y score is related to the anterior direction and a negative Y score to the posterior direction. The same score is calculated with the mediolateral signal and called the X score. A positive X score is related to the right direction and a negative X score to the left direction.
Then the inverse mean of the score in each direction (anterior, posterior, right and left) multiplied by 100 was calculated (c).
A final composite score (CS) was calculated for each type of sensorial stimulation. The CS was the mean score for each test type (2 tests for the proprioceptive stimulation, 4 for the visual stimulation). the mean score of each test for one type of sensorial stimulation. The higher the CS, the less the participant is sensitive to the stimulation. This score was based on a previously published CS (15), except that we used the inverse of the original CS to be able to include falls being scored as 0.
During the evaluation, a fall was considered as each time the assessor had to touch or catch the participant to avoid a real fall. If a fall occurred during a test, the score was equal to 0.
Classification of participants was similar to that previously defined (15). The threshold of the 25th percentile in the CS for controls was used to define sensitivity to a sensory stimulation. A participant with a CS lower than the 25th percentile for the control CS was considered sensitive to that type of stimulation and one with a CS lower than the 10th percentile, highly sensitive.
GraphPad Prism v6 was used for data analysis. Data are given as mean and standard deviation (SD). The normality of data distribution in CSs was tested by the Shapiro-Wilk normality test. Unpaired t-test was used to compare CSs between patients with CADP and controls. The Mann–Whitney test was used to compare the Romberg score between patients with CADP and controls. Correlation between sensitivity impairment and visual CS between sensitivity impairments and proprioceptive score were analysed by the Spearman’s correlation coefficient. Fischer’s test was used to compare the sensitivity (defined by the sensitivity score) between patients and healthy controls. Receiver operating characteristic (ROC) curve analysis involved calculating the area under the ROC curve (AUC) and sensitivity and specificity. The ROC curves for visual and proprioceptive CSs were used to compare AUCs between the 2 CSs. The paired z-score was calculated as z=|AUC1–AUC2|√(SEAUC12+SEAUC22), and 95% confidence intervals (95% CIs) were estimated. p < 0.05 was considered statistically significant.
The study was approved by the ethics committee (reference 2013-A00997 for patients with CIDP and reference 2014-A01068-39 for patients with anti-MAG neuropathy). Patients gave their informed consent to be included in the study.
Twenty-five patients with CADP (13 CIDP, 12 anti-MAG neuropathy) and 25 healthy controls (mean) age 64.5 years (SD 16.5), range 26–88, vs 57 (SD 11.8), range 37–82, no age-matching) were investigated. Tables I and II show the characteristics of participants. Mean time since CADP diagnosis was 4 (SD 4) years (range 0–18 years). Major complaints of patients with CADP were perception of gait instability (68%) and paraesthesia (60%). Motor deficit was minimal for patients with CADP (mean MRC 48 (SD 3); range 40–50). Sensitivity was impaired for patients (mean 5.8 (SD 2.5); range 2–10) (Table I).
Table I. Characteristics of patients with chronic acquired demyelinating polyneuropathy (CADP) and healthy controls
Table II. Demographic and clinical data for 25 patients with chronic acquired demyelinating polyneuropathy (CADP)
Twenty-five patients with CADP (13 CIDP, 12 anti-MAG neuropathy) and 25 healthy controls (mean) age 64.5 years (SD 16.5), range 26–88, vs 57 (SD 11.8), range 37–82, no age-matching) were investigated. Tables I and II show the characteristics of participants. Mean time since CADP diagnosis was 4 (SD 4) years (range 0–18 years). Major complaints of patients with CADP were perception of gait instability (68%) and paraesthesia (60%). Motor deficit was minimal for patients with CADP (mean MRC 48 (SD 3); range 40–50). Sensitivity was impaired for patients (mean 5.8 (SD 2.5); range 2–10) (Table I).
Patients with CADP and controls significantly differed in mean statokinesigram area with eyes open (306.9 (SD 236.5) vs 152.1 (SD 116.3), p = 0.001) and even more with eyes closed (1,051 (SD 2,010) vs 212 (SD 144.1), p < 0.0001). The mean Romberg score did not differ between patients and controls (279.4 (SD 226.6) vs 183.8 (SD 135.7), p = 0.11).
The CSs for each participant and visual and proprioceptive stimulation are shown in Fig. 1. Patients and controls were ranked from high to low CS for both stimulation types. The lower the CS, the more sensitive the participant was to the stimulation. No score means the patient fell with each test of a sensory stimulation.
Fig. 1. Composite scores ranked from high (less sensitive) to low (more sensitive) for patients with chronic acquired demyelinating polyneuropathy (CADP) and healthy controls with (A) proprioceptive or (B) visual stimulation. Score of 0 means falls for all tests. The lower the score, the more sensitive the patient.
Visual input. As expected, patients with CADP were more sensitive to visual stimuli than were healthy controls. Mean CSs for optokinetic stimulations were significantly lower for patients than controls (10.5 (SD 8.7) vs 22.9 (SD 7.5), p < 0.0001) (Fig. 2). For each direction, healthy controls were disturbed in the expected direction for each test, whereas CADP patients always had a higher score in the anteroposterior direction, even for the rightward or leftward stimulation.
Fig. 2. Mean composite score for patients with chronic acquired demyelinating polyneuropathy (chronic acquired demyelinating polyneuropathy; CADP) and controls with visual and proprioceptive stimulation. Data are mean (and standard deviations). **p < 0.01, ****p < 0.0001.
There were 29 falls among 100 tests in 13 different patients with CADP, and only 4 falls in 4 different healthy controls.
According to the “sensitivity score” as defined, 22/25 patients with CADP were sensitive to optokinetic stimulation (CS < 19.2), 16/22 being very sensitive (CS < 13.3) (Table III). As defined, 6/25 controls were sensitive to visual input, 2/6 being very sensitive. Conversely, 3 patients with CADP were insensitive (CS > 19.2) compared with 19 healthy controls. This difference in visual sensitivity was significant (p < 0.0001, Fisher’s test).
Table III. Number of patients with chronic acquired demyelinating polyneuropathy (CADP) and healthy controls sensitive or not to visual and proprioceptive stimulation
Proprioceptive input. Mean CS for tendon vibration was significantly lower for CADP patients than for controls (13.9 (SD 4.8) vs 18.4 (SD 4.8), p = 0.002) (Fig. 2). Moreover, 4 falls occurred during 50 tests for 3 different patients with CADP, with no falls in healthy controls.
According to the “sensitivity score” as defined, 17/25 patients with CADP were sensitive to vibratory stimulation (CS < 15.9), 9/17 being very sensitive (CS < 11.3) (Table III). As defined, 6/25 controls were sensitive to proprioceptive input, 2/6 being very sensitive. Conversely, 8 patients were insensitive (CS > 15.9) compared with 19 healthy controls. This difference in proprioceptive sensitivity was significant (p = 0.004, Fisher’s test).
Although we had an age-matching control group, the number of participants aged > 70 years was higher for patients with CADP than controls (12 vs 3). The CS for patients with CADP aged > 70 and < 70 years was compared and no significant differences were observed in proprioceptive stimulation (mean CS 14.9 (SD 1.3) vs 11.5 (SD 1.7), p = 0.129) or visual stimulation (12.8 (SD 9.5) vs 7.2 (SD 7.7), p = 0.145).
No significant correlations between MRC score and mean visual or proprioceptive CS were found. This can be explained by the relatively conserved motor strength for most of our patients. A correlation was found between sensitivity impairment and mean visual CS (r = 0.48, p = 0.02) (Fig. 3), but not between sensitivity impairment and mean proprioceptive CS.
Fig. 3. Correlation between proprioceptive composite score and sensitivity impairment (r=0.26; p = 0.23). Correlation between visual composite score and sensitivity impairment (r=0.48; p = 0.02).
Fig. 4 shows the ROC curve for visual and proprioceptive CSs. Table IV shows the discriminative properties in terms of AUC, sensitivity, and specificity of these variables.
Fig. 4. Receiver operating characteristic (ROC) curve analyses of visual and proprioceptive composite scores for patients with chronic acquired demyelinating polyneuropathy (CADP) and controls.
Visual ROC curve. The optimal cut-off CS for patients with CADP was 19.4, with AUC 0.85 (95% CI 0.74–0.96, p < 0.0001) and sensitivity 0.88 (95% CI 0.69–0.97). Specificity was 0.76 (95% CI 0.55–0.90) (Table IV).
Proprioceptive ROC curve. The optimal cut-off CS for patients with CADP was 15.6, with AUC 0.75 (95% 0.61–0.88, p = 0.003) and sensitivity 0.64 (95% CI 0.43–0.82). Specificity was 0.8 (95% CI 0.59–0.93) (Table IV).
Comparison of the derived ROC curves showed that the AUC did not differ significantly between visual and proprioceptive CSs (Z = 1.14, p = 0.3).
Table IV. Receiver operating characteristic (ROC) curve analysis of predictive value of visual and proprioceptive composite scoresa
The aim of this study was to investigate the weight of visual and proprioceptive inputs measured indirectly in the standing position in patients with CADP and in healthy controls. On stimulating proprioceptive and visual sensory systems by using tendon vibrations and an optokinetic device with participants standing on a double force platform, patients were found to be more sensitive to visual stimuli and to proprioceptive stimuli than were healthy controls.
As expected, patients with CADP were more sensitive to visual stimulation than were controls. Visual control is known to be crucial in determining balance in polyneuropathic disease. Several studies reported that, with reduced visual information, patients with sensory deficits have a greater tendency to fall spontaneously (18, 19). Equilibrium performance in dynamic posturography was lower for patients with polyneuropathy than healthy participants under conditions of absent vision, sway-referenced surroundings and sway-referenced platform and surroundings, but did not differ from healthy participants when both the platform and visual surroundings were stable (20). A recent study presented similar results evaluating static balance with open and closed eyes on a Wii balance board in patients with type 2 diabetes mellitus associated or not with polyneuropathy: patients with associated polyneuropathy showed altered balance and worse static balance than those without polyneuropathy, especially with eyes closed (21). Therefore, elimination of visual stimulus affects postural control.
However, contrary to expectations, our patients with CADP also showed proprioceptive sensitivity, despite the sensory impairment due to the disease. Other
authors have observed such results (22) with proprioception stimulation produced by another method (ankle movement) in older patients with polyneuropathy. The authors observed no differences in the weight of proprioceptive information between older participants without and with polyneuropathy, in contrast to the expectation that the latter participants would rely less on a deficient sensory channel.
The greater visual sensitivity of our patients vs controls does not necessarily mean that a patient depends on this sensory input. Indeed, visual dependence is defined as the preponderance given to visual cues, even when incorrect, despite normal vestibular and proprioceptive cues (23). In our study, many patients were sensitive to visual input, but many were also sensitive to proprioceptive input, which suggests that, despite the neuropathy, the proprioceptive system is still efficient, so they would not be systematically obliged to rely on vision when a sensory conflict occurs. The same behaviours observed in post-stroke patients (15, 24) has led to preferring the term “sensitivity” rather than “dependence,” which does not describe exactly the same behaviour. Hence, in daily activities, some patients are assumed to have developed a useless compensatory visuo-dependent behaviour.
The sensitivity to proprioception stimulation despite the proprioceptive impairments in our patients with CADP is questionable. In these patients, this focal vibration applied to tendons is perceived and treated despite clinical proprioceptive impairment. However, we cannot exclude that propagation of this focal vibration through the different tissues (muscles, tendons, bones, skin etc.) could stimulate proprioception at another less-deficient level (25). We can assume that if a rehabilitation programme for visual deprivation has a positive effect on balance and walking, this argues for a not-adapted visuo-dependent behaviour.
In this study, ROC curve analysis enabled us to define a cut-off able to discriminate sensitive and non-sensitive patients.
No significant differences were observed between patients with CADP and controls in the Romberg quotient. Although the Romberg is a classical test in clinical practice to detect proprioceptive impairments, this lack of significant decrease in stability with eyes closed has been described previously (12). However, we noticed that the area of CoP displacement with eyes open and eyes closed was significantly higher for patients with CADP than for controls. The large surface area of CoP displacement with eyes open for patients with CADP could account for the absence of significant increase in surface area with eyes closed vs eyes open (i.e. the Romberg coefficient). This observation also accounts for the effectiveness of the residual proprioception.
Some limitations of our study must be highlighted. The number of participants included was rather low, but the disease is rare. We found a difference in sex between groups, but no difference in CS by sex in controls and patients. We also requested only one attempt for each test because of fatigue related to the length of the experiment, which could question the reproducibility of our results. The choice of the vibratory frequency of 50 Hz is questionable. We retained this frequency from the previous work on post-stroke patients (15). Although the best frequency to stimulate proprioception is between 70 and 80 Hz (26), we considered that 50 Hz would be less disturbing. In addition, the number of participants aged > 70 years was higher for patients with CADP than for controls, which could influence the results because of the usual proprioceptive impairments in older people. However, we did not observe differences between the 2 categories of age in proprioceptive and visual CS.
To conclude, we found patients with CADP to be sensitive, as expected, to visual information for controlling their standing posture at rest, but contrary to expectations, they were also sensitive to proprioceptive stimulation, despite clinical impairments. These interesting new data offer a new perspective for designing a rehabilitation programme for these patients to improve balance by promoting the use of proprioceptive inputs, thereby reducing visual dependence (13, 27, 28).
This study is supported by Assistance Publique - Hopitaux de Paris Promotion.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize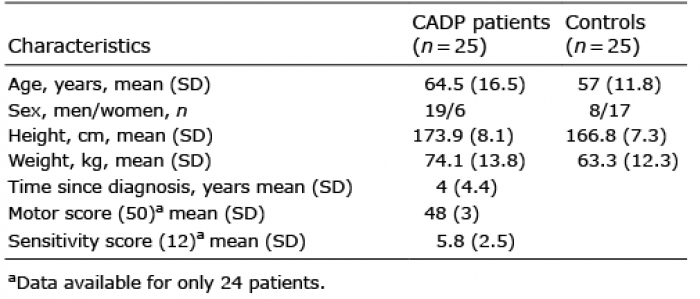 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize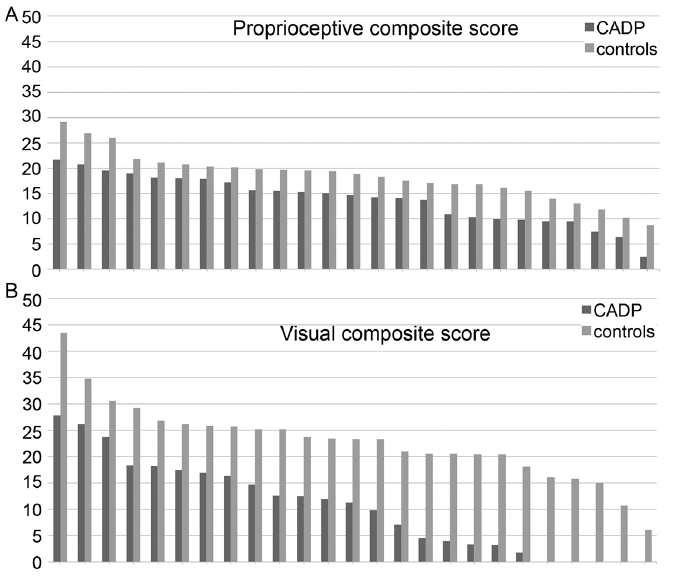 Click to show fullsize
Click to show fullsize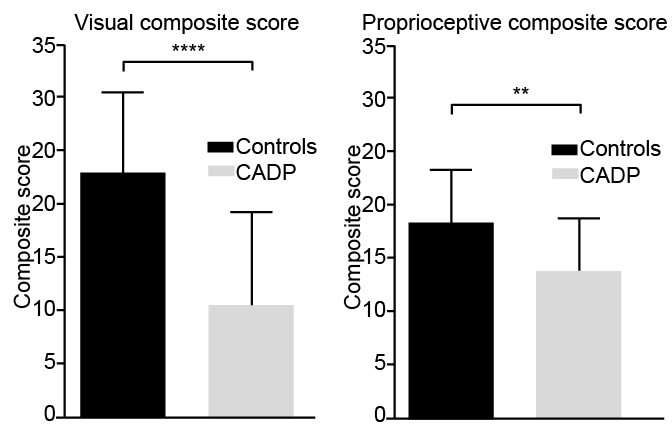 Click to show fullsize
Click to show fullsize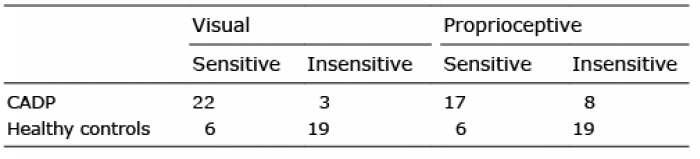 Click to show fullsize
Click to show fullsize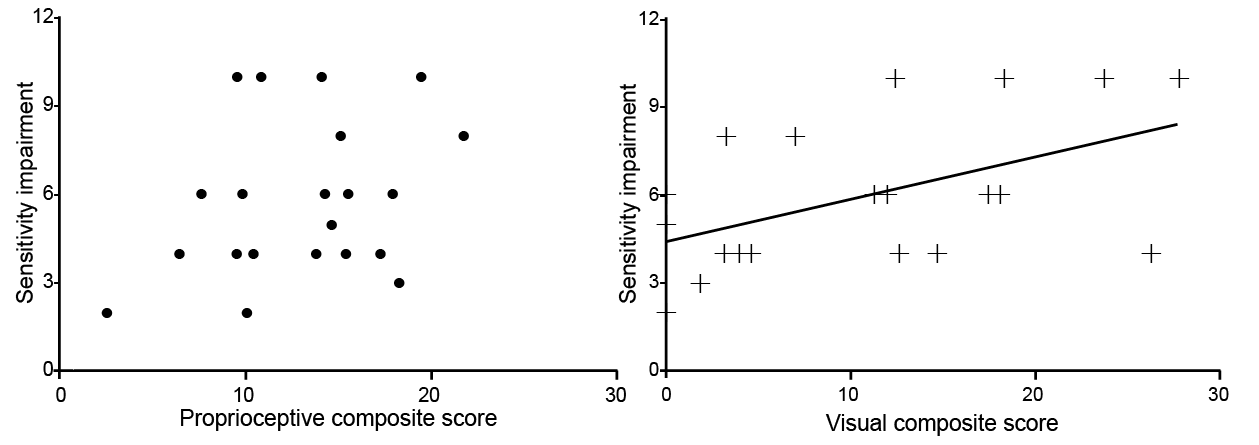 Click to show fullsize
Click to show fullsize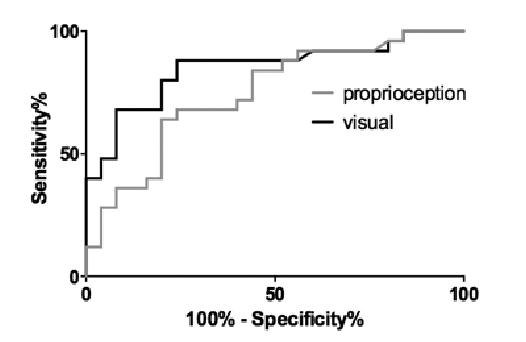 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize